Our highly
effective Program
Reduce costs and improve result with a risk-free alternative to additional surgery
Stretch Education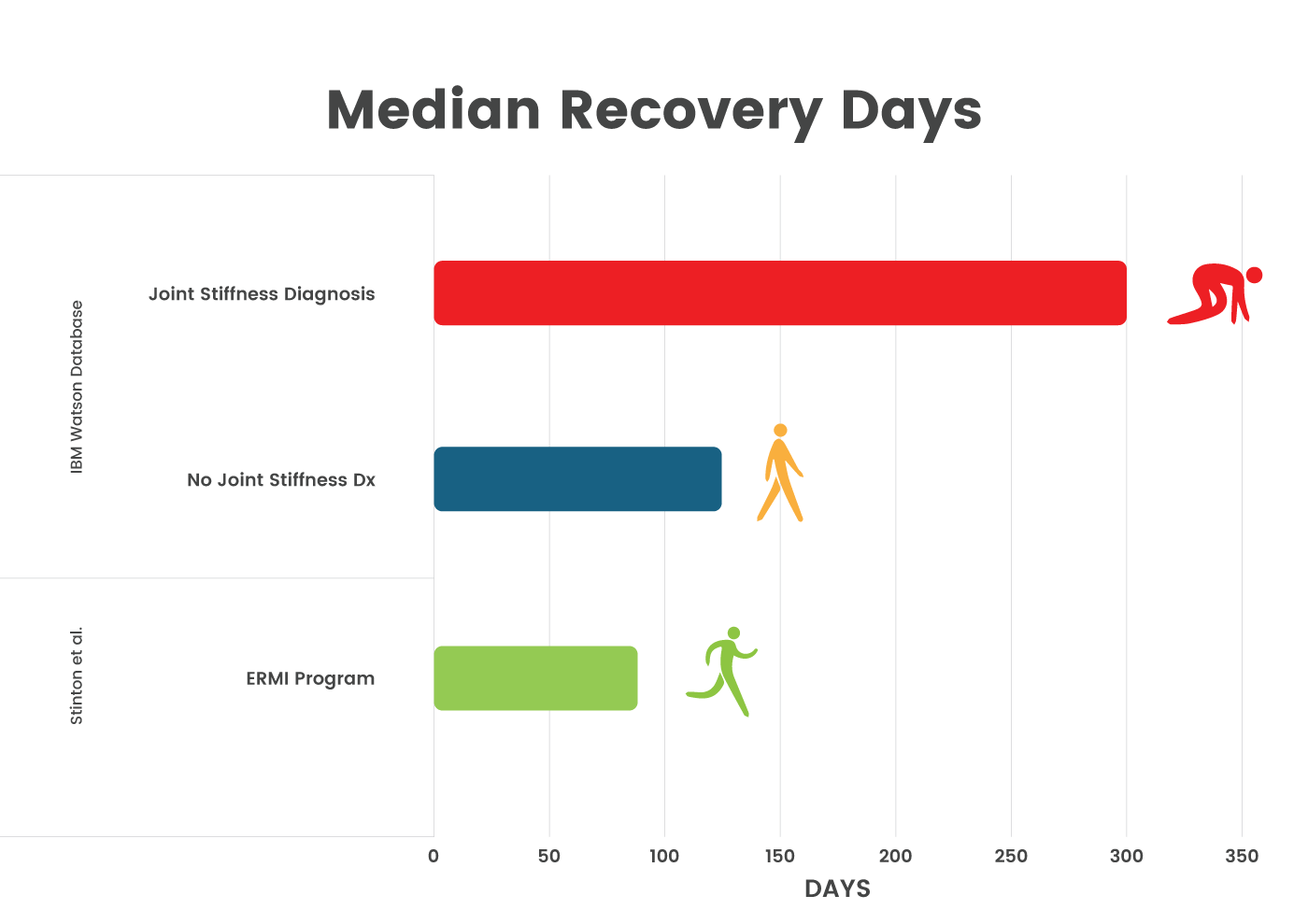
The ERMI Program started at 6 weeks has motion recovery by 3 months post-op*
 Flexionater?
Flexionater? 
| Ermi Flexionater 42 hours at 1 hour/day* | 4 PT visits per week at 1 hour stretch/visit | 4 PT visits per week at 30 min stretch/visit | |
| Time to Recover | 42 days | 74 days | 148 days |
| Physical Therapy CPT 97140 for Manual Therapy Mean Medicare Fee Schedule 2024 | Stretch Lab or Stretch Zone | IBM Watson Database | Stretch Zone/Lab Treatment Costs | Physical Therapy Costs | ||||
| 15 min session | 1 hour session | 1 hour per day for 1 month | 1 hour session | 1 hour per day for 1 month | Accumulative Risk of MUA Surgery | Avg Total of 42 hours* | Avg Total of 42 hours* | |
| Retail costs of a Knee Recovery Stretch Program | $26.52 | $106.08 | $3,182.40 | $126.00 | $3,780.00 | $11,389.75 | $6,132 | $5,295.36 |
The ERMI Program started at 6 weeks has motion recovery by 3 months post-op*
The science of stretching and the use of stretching assist devices or splints was first explored by Hippocrates (460-377 BC) in “Codex Laurenzianus LXXXIV,7” (Biblioteca in Firenze, Italy). By the early 1800s the Swedish Gymnastik discipline was reporting the use of manual stretching therapy as a part of a rehabilitation program. By 1874, Dr. Andrew Taylor introduced the Science of Osteopathy which utilizes passive stretching of the soft tissues to restore normal structure and function. Specialized stretching techniques to facilitate the improvement of joint motion or flexibility were developed in the mid 1900s. One technique called Proprioceptive Neuromuscular Facilitation (PNF) was developed at the Kabat-Kaiser Institute from 1946 to 1951 by neurophysiologist Herman Kabat and physical therapist Margaret “Maggie” Knott. By the early 1980s motion loss secondary to joint stiffness was considered an orthopedic epidemic, particularly after knee replacement or ligament surgery.
In response to this epidemic the orthopedic community turned to a device invented in Toronto, Canada called the Continuous Passive Motion (CPM) machine, which was intended to help treat “intra-articular fractures”. It was hoped that by placing patients on a CPM immediately after surgery that the continuous motion would help mitigate the motion loss due to joint stiffness. By the early 2000s, research showed that pre-emptive continuous passive motion using a CPM machine could not substitute for stretching in the post-operative period. Stretching and/or the use of stretch assist devices or splints remain the cornerstone of range of motion recovery for motion loss due to joint stiffness and cannot be considered experimental or investigational. Stretching by a Physical Therapist is covered by all insurance companies under CPT code 97140. Stretch assist devices or home mechanical therapy devices/splints are simply a different delivery form for post-operative stretching than by a Physical Therapist.




With the Ermi program, you will reduce the need for costly revision surgeries and in-hospital treatment and decrease the number of disability payouts by getting your clients back to work faster. Ermi programs can save the healthcare system over $8,000 per patient compared to similar products.**
With more than 150,000 patients treated, the Ermi program is More than 90% effective in recovering range of motion within 3 months and preventing motion restoring surgery.*
Strict compliance and use protocols ensure that only patients who need our solution receive it, and our Ermi professionals monitor patient progress to avoid overuse.
Sources:
* Papotto BA, Mills T. Treatment of severe flexion deficits following total knee arthroplasty: a randomized clinical trial. Orthopedic Nursing. 2012 Jan-Feb; 31(1):29-34.
** Stephenson JJ et al. Knee-attributable medical costs and risk of re-surgery among patients utilizing non-surgical treatment options for knee arthrofibrosis in a managed care population. CRMO. 2010; 26(5):1109-1118.
Aspinall et al. Journal of Orthopaedic Translation 2021. Medical stretching devices are effective in the treatment of knee arthrofibrosis: A systematic review.
Papotto, Orthopaedic Nursing, 2012. Treatment of severe flexion deficits following total knee arthroplasty: A randomized clinical trial.
Stinton, Journal of Orthopaedic Surgery and Research, 2022. Efficacy of non-operative treatment of patients with knee arthrofibrosis using high-intensity home mechanical therapy: a retrospective review of 11,000+ patients.
Yenchak et al. Journal of Orthopaedic & Sports Physical Therapy 2011. Criteria-based management of an acute multi-structure knee injury in a professional football player: a case report.
Uhl and Jacobs, Sports Health, 2012. Torque measures of common therapies for the treatment of loss of knee flexion.
Stephenson et al. Current Medical Research & Opinion 2010. Knee-attributable medical costs and risk of re-surgery among patients utilizing non-surgical treatment options for knee arthrofibrosis in a managed care population.
Dempsey, et al. Sports Medicine, Arthroscopy, Rehab Therapy & Technology, 2010. High-intensity mechanical therapy for loss of knee extension for worker’s compensation and non-compensation patients.
Heckmann – GATA Symposium Presentation, 2007. Treatment of arthrofibrosis following total knee replacement using high-intensity stretch mechanical therapy devices.
Wilk et al. Cartilage 2010. Rehabilitation following microfracture of the knee.
Branch – American Journal of Orthopedics, 2003. Mechanical therapy for loss of knee flexion.
Stinton, et al. Journal of Orthopaedic Surgery and Research, 2022. Efficacy of high-intensity home mechanical stretch therapy for treatment of shoulder stiffness: a retrospective review.
Wolin, et al. Annals of Physical Medicine and Rehabilitation, 2016. High-intensity stretch treatment for severe postoperative adhesive capsulitis of the shoulder.
Teytelbaum et al. BMC Musculoskeletal Disorders, 2024. Efficacy of a high-intensity home stretching device and traditional physical therapy in non-operative management of adhesive capsulitis – a prospective, randomized control trial.
Dempsey, et al. American Journal of Physical Medicine and Rehabilitation, 2011. Maximizing total end range time is safe and effective for the conservative treatment of frozen shoulder patients.
Beckley, et al. Submitted to the Journal of Orthopaedic Surgery and Research, 2024. Evaluating the effectiveness of high-intensity mechanical stretching devices in treating ankle stiffness: a retrospective case series analysis.
Jacobs and Sciascia, Sports Health, 2011. Factors that influence the efficacy of stretching programs for patients with hypomobility.
Davies and Ellenbecker, BioMechanics, 1999. Focused exercise aids shoulder hypomobility.
All products are FDA Approved
If you have a question, concern, or issue, please fill out the short form and we will have an Ermi representative get in touch with you.
© 2024. All Rights Reserved by ERMI